Contents
- Introduction
- What is Occlusion training
- Physiological Mechanisms
- Protocolls researched
- Summary
- References
Introduction
Before going into the physiological mechanisms of Blood Flow Restriction and its practical appliance, lets see what this method is and how it is defined.
Blood is responsible for the transport of oxygen, nutrients, and many other molecules crucial for sustained life. An entire category of supplements has emerged in the past decade, focused on increasing blood flow and thus intending to enhance anabolism. What if though the opposite may be true. What if, lets say, someone tells you that occluding blood flow to muscles can have an anabolic effect?
Occlusion training, scientifically known as “blood flow restriction training” (BFR), involves restricting/reducing blood flow in the veins of a working muscle/area to elicit gains in size and strength. By reducing venous return occurs venous pooling.
It was originally developed by Dr. Yoshiaki Sato in 1966 when he first came up with the idea. Between 1967-1974 he was conducting uncontrolled experiments on himself and later on in controlled experiments in Japan developing this type of training he called Kaatsu training.
Of course, like anything, it only works if you do it right so let’s talk about the how and why.
What is Occlusion Training?
BFT or occlusion training, involves basically decreasing blood flow from a muscle (occluding veins) by the application of a pneumatic wrapping device around the proximal part of the target muscle. The goal is to prevent blood flow return from the muscle, causing the blood to pool in the muscle (i.e. you do NOT want to restrict the arterial blood flow to the muscle, only the venous return from the muscle). Several scientific papers have hypothesised that BFR increases muscular strength and hypertrophy through a variety of mechanisms including metabolic accumulation, fast-twitch muscle fiber recruitment, increased protein synthesis and cell swelling.
A big issue with this type of training is that using pneumatic wrapping devices (ie modified blood pressure cuffs) is expensive and not accessible or practical to use outside of a laboratory environment. The effectiveness of practical BFR using either the KAATSU devise or inexpensive elastic wraps has been researched over the last 3 years which introduces a new concept for rehabilitation for physiotherapists.
Physiological Mechanins
There are at least three ways that BFR works.
A) Fiber Type Recruitment
Slow twitch fibers (oxidative) are primarily recruited during low intensity exercise, as they are able to adequately handle the workload. This isn’t optimal to big muscle gains/growth because, fast twitch fibers (glycolytic) have the greatest potential for growth. When one moderately restricts blood-flow, it limits the amount of oxygen available to the slow twitch (oxidative) fibers thus resulting in a rapid recruitment of fast twitch (glycolytic) fibers perform the the workload. In other words that means that with occlusion fast twitch fibers are able to be trained with a low-intensity workload. EMG (electromyography) studies conducted the last years have confirmed that there is an increase in motor unit firing with BFR. The EMG data also revealed no difference between low intensity BFR training and high intensity exercise. Thus training BFR with light weight mimics mimics the firing rate of that of heavy resistance training.
B) Metabolic Accumulation
Further research on BFR training with low intensities has shown increases in lactate and growth hormone (GH). In fact in experimental studies it has been shown that the increase in GH has actually been shown to be even higher than that registered with heavy resistance training. A study performed in athletes showed a 290x increase in GH compared to baseline. Due to the fact that there is an inverse relationship between Lactate and pH, so as lactate increses, pH decreases. That makes the cellular environment more acidic, which is linked to increased GH, by stimulating the pathway that plays an important role in the secretion of GH.
C) mTOR Pathway
The mTOR pathway, responsible for protein synthesis, has also been shown to be activated with low intensity BFR training. In the study of Fujita et.al phosphorylation of S6k1 was increased by three-fold following BFR training and remained elevated at 3 hours post exercise. Such an increase in protein synthesis is primed for muscle growth.
Summarizing: Fast twitch fiber recruitment, metabolic accumulation, and mTOR activation are three of the most dominant mechanisms involved in the muscle growth effects seen with BFR training. Others that likely play some role, include Heat Shock Proteins, NOS-1 and decreased expression of myostatin.
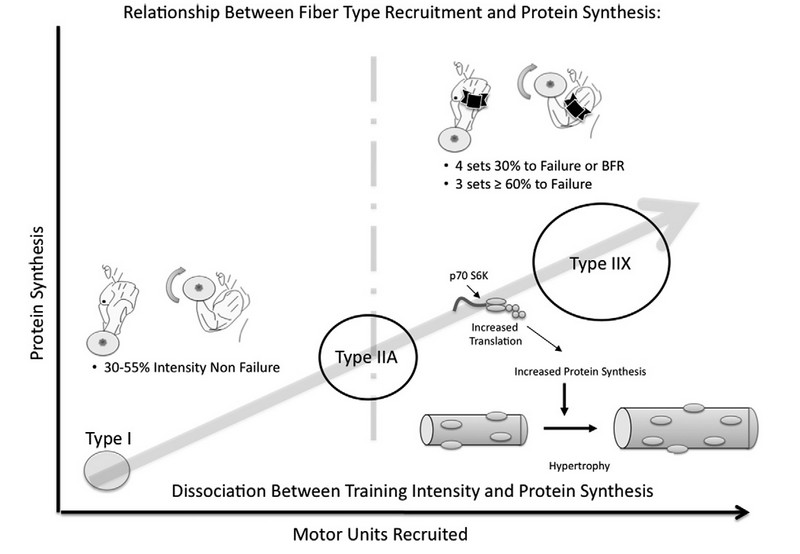
The relationship between exercise volume, motor units recruited, and protein synthesis. As intensity increases from 30–55% of one’s repetition maximum the higher threshold motor units are recruited. Once a certain amount of volume has been reached, as indicated by the threshold marker in the center of the figure, maximal protein synthesis from exercise will occur. This occurs independent of exercise intensity provided the metabolic stress and/or volume is adequate to recruit the highest threshold motor units.
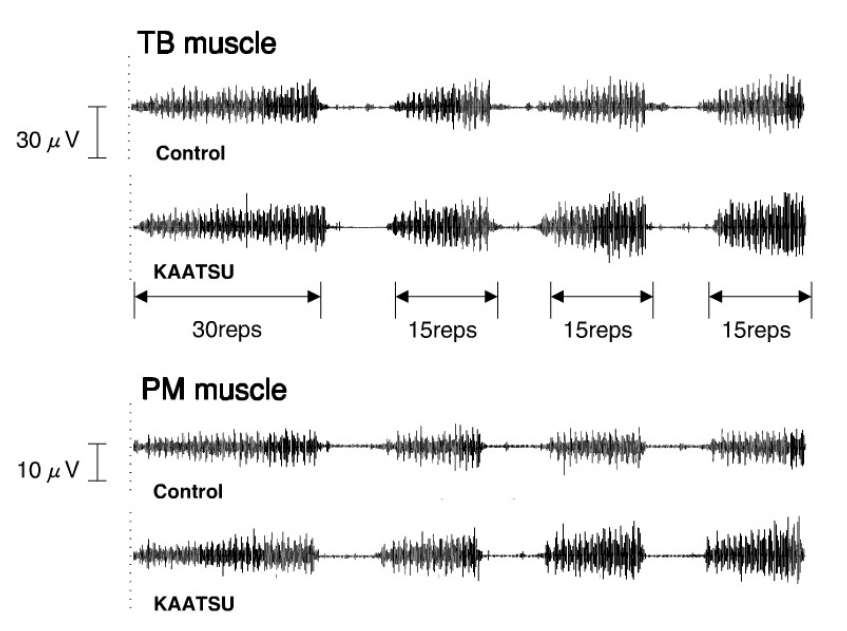 Typical examples of EMG signals recorded from triceps branchii and pectoralis major muscles during low-intensity flat bench press exercise with and without KAATSU.
Typical examples of EMG signals recorded from triceps branchii and pectoralis major muscles during low-intensity flat bench press exercise with and without KAATSU.
3) Protocols researched and Results
BFR WALKING vs BFR LIFTING
A study performed by Loenneke and collegues published an extensive research paper on BFR in which numerous BFR topics were analyzed to determine what works best. BFR during walking was compared to a lifting at 20-40 percent of an individual’s 1RM. Results indicate that BFR lifting was more effective than BFR walking. One should take into account, that when lifting is not feasible or as a further stimulation, BFR walking can be an alternative. It can because of injury or familiarization to technique before progressing to lifting. This is due to the fact that in the BFR walking group was also registered muscle gain.
BFR CONCENTRIC vs BFR ECCENTRIC
Study done by Thiebaud investigated the proper contraction type for BFR. While the eccentric (lowering) movement type causes most growth during traditional heavy lifting, the opposite was found during the BFR. It was conducted that the concentric phace (pumping), flood the mscle with fluid and lactate and can cause most growth.
PRACTICAL BFR TRAINING vs KAATSU DEVICE BFR TRAINING
Several studies have attempted to simplify the technique by making it available for the majority of Physiotherapists and Sport Science specialist. This has been called practical BFR training as it is uses warps (thigh,knee,wrist) lowering significantly the cost used for the equipment. In a study og Wilson it was found that just like the KAATSU device BFR, practical BFR could drastically increase muscle cell swelling, muscle fiber recruitment, as well as blood lactic acid levels.
Another study by Lowery, showed the efficacy of the method recently in an 8-week study in which he found that practical BFR could cause the same types of gains that were achieved with the KAATSU device BFR.
Yamanaka and Luebbers also showed the effectiveness of Practical BFR training (20% of 1RM) on muscular strength assessed by 1RM change in collegiate athletes (n=16 and n=62 respectivelsy).
Another comprehensive study by Wilson assessed young males (n=12) performing leg press at 30% of 1RM for four sets using different practical BFR conditions.The control= 0/10 pressure and moderate pressure= 7/10 subjective perceived wrap tightness. The amount of practical BFR was quantified by ultrasonography: a)at a moderate perceived wrap tightness (7/10) complete venous occlusion occurred but not arterial and b) at a perceived wrap tightness of 0/10 no BFR occurred. Their results showed that blood lactate, quadriceps cross-sectional area (MRI) and knee extensor muscle activity measured by EMG (mV) significantly increased in the moderate tightness (7/10) practical BFR group, with no change in the control group (0/10).
This study with 7/10 perceived tightness BFR has been repeated by Lowery who performed a crossover study (n=20) for the elbow flexors at a) 30% of 1RM for 30 repetitions, 7/10 tightness or b) 60% of 1RM for 15 repetitions (0/10 tightness) for four weeks, for a combined 8-week training duration.
Researchers showed that both practical BFR training and 60% of 1RM training led to significant increases in bicep hypertrophy (ultrasonography), with no differences in hypertrophy gains.
CONS of the above studies is that exercise technique (range of motion or contraction speed) was not described or standardised. This can result in bias as some subjects have varied times under tension which in turn effect the strength gains observed.
Blinding of the outcome assessors only occurred in the Lowery study which could lead to added encouragement given to the practical BFR subjects especially during maximal strength testing, possibly effecting the results.
The current research on practical BFR suggests that it could provide similar benefits to using KAATSU devise but that is certainly not definitive yet. On the other hand one should take into account that it is still a possible option for elderly and also post surgical patients who cannot tolerate heavy loads to aid in increasing their strength and ultimately function due to it being implemented sooner in their rehab process and possibly speeding up their recovery. A method such as practical BFR is easily available and cost effective.
BFR BODYWEIGHT vs BFR 20-30% of 1RM
Although some papers have registered positive results in terms of muscle gains and strength by using body weight BFR, the majority of the research have suggested that loads of 20-30% of 1RM, 15-30 reps with 30-60 sec rest between sets, has been supported by meta analytical data and evidence based training guidelines to significantly increase strength from the elderly to elite athletes.
NO SATO-KATSSU RESEARCH
By reading through basically all the literature done on BRF training, it was shown that much of it was conducted by Professor Sato and hus KAATSU training university. Although those researches done may be legitimate and comprehensive, excluding such a possibility of bias, any research performed by Sato and his team has been excluded in this paragraph.
Despite some few studies, mentioned below, concluding with either no difference between between BFR and traditional training or traditional training being superior to BFR, the majority of the research has showed superior effects of BFR on muscle gains and strength, but not necessarily bone formation or passive tissue development.
– Study by Madarame showed that while occlusion training improved muscle strength and size, it did not improve jump performance in previously untrained young men.
– Study by Kim demonstrated that low intensity resistance training with BFR was less effective than high intensity resistance training for eliciting bone formation and muscle hypertrophy responses.
– Traditional training also proved to be much more effective for bone turnover than blood flow-restricted training in Kims study.
Occlusion training is thought to work through the process of “metabolic accumulation.”
Basically, instead of letting your body flush all the metabolic products of exertion through the system, the tourniquet keeps it all in the area. This stimulates a big release of anabolic growth factors, recruits more fast-twitch fibers, and induces more production of protein. Moore conducted a study that showed vascular occlusion training increased muscle strength and changed some aspects of neuromuscular function that conventional training did not.One Japanese study performed in 1999 even showed a 290-times increase of growth hormone levels in occlusion-users, and those levels remained slightly higher than the control level after 24 hours.
Occlusion training also seems to stimulate the production of heat shock proteins, which monitor cell proteins and help transport other proteins across cell membranes, aiding in cell repair. Occlusion training appears to affect Nitric oxide synthase-1 (which helps control blood pressure, insulin secretion, blood vessel growth, and peristalsis, and helps catalyze nitric oxide from L-arginine) and reduces myostatin as well (animals lacking myostatin have larger muscles than other animals). More research is needed on the exact mechanisms of occlusion training, but it seems to have many avenues through which it works its magic.
3.1) Upper and Lower Extremities
Occlusion benefits for the lower extremities have been very promising, in that every study has shown significant increases in muscle mass, strength and neuromascular firing, and almost all have registered results over the control group. I refer to the studies mentioned earlier of which the majority are performed on the lower extremities.
Use the following equation to estimate your min and max intensity:
Minimum Intensity Equation = Your One Repetition Maximum X 0.2
Maximum Intensity Equation = Your one Repetition Maximum X 0.5
For example, if you’re 1RM on the Squat is 200 kg, that means:.
200 x 0.2= 40kg would be the minimum weight you would work with.
200 x 0.5=100kg would be the maximum weight you would work with.
Table 1. Lower body Recommendations Sets/Reps 3/10, Rest 1-2 min, Intensity 50% 1RM
– BB Squat
– Leg press
– Leg extension
– Leg Curl
– Hack squat
– Romanian Deadlifts
– Calve raises (toes in-out modifications)
As far as occlusion for the upper body, one can achieve direct BFR for the m.triceps brachi, m.biceps brachi and the other upper/lower arm muscles. When it comes to the torso, that can happen indirectly by first fatiguing the triceps following bench press or pushups, or biceps following flyes, pull down or rowing. A research conducted by from Madarame has shown that one can receive benefits of occlusion for the upper body by occluding the lower body. This cross-over effect is likely attributed to the large increase in hormones due to the larger muscles of the leg musculature. Those hormones are transported superiorly to the upper body through the blood steam. The larger quadriceps will increase hormones more so than the smaller biceps. This particular study showed that when occlusion of the legs followed a light upper-body exercise, it resulted in significant hypertrophy.
Table 2. Upper body Recommendations Sets/Reps 3/10, Rest 1-2 min, Intensity 50% 1RM
– BB Bench press
– BB Military
– BB Curl
– BB Row
– Lat pulldown
– DB Triceps Extensions
– Dips
*Madarane protocol: when you have finished the exercise, you wrap your legs and perform 3 sets of leg extension and/or 3 sets of leg curls. The intensity of the leg extension/leg curl is set at 3 sets of 20-30% of 1RM on leg extension/leg curl. Reps are set at 30-15-15 with 30 seconds to 1 minute rest between each set. Here’s an example of how it would look for the bench.
- Bench Press your 3 sets at 50-60% of 1RM
- Wrap your legs for 3 sets of 30-15-15 at 30% 1RM on leg extension with 30
- Take the wraps off and wait for ~5 minutes to restore blood flow
- Wrap your legs again for 3 sets of 30-15-15 at 30% 1RM on leg curl with 30 seconds-1 minute rest.
- Take off wraps
Summary
- There is strong evidence that BFR is quite effective, but it should be performed by proffesionals.
- As any type of training, it does not replace, but rather complement.
- Positive effect on muscle tissue, but not on passive tissue or bone formation.
- Preferably do not BFR for more than 30min, purely for safety concern, 1-3 times a week for around 4-6 weeks. Begin by implementing 1 exercise as BFR before progressing. It is important to distinguish between acute and chronic effects of BFR, as the acute effect is definite positive effekt, but cutting off blood flow can result in tissue damage.
- Do not BFR above 50% as this DO NOT give superior effects.
- Ask for professional help from a physiotherapy or sport science practitioner to make sure you get the desired effect. It is easier to adjust the tightness of the wrap, or even have a practitioner with a KAATSU devise.
- SEE CONTRAINDICATIONS below for underlying pathologies.
In light of available research on the effectiveness of occlusion training, it would appear there is benefit to it for both strength and hypertrophy gains for lifters and rehabilitation. It’s important to note, though, that occlusion training is not meant to replace heavy lifting. It should be seen as complementary tool to exercise or used as therapy for those who cannot lift heavy weights. It’s great for deloading periods or on lighter training days.
4.1) Special Populations
– Atheltes: variation, reduced mechanical load, rehabilitation
– Elders: Rehab, low mechanical load and muscle hypertrophy
Improving someone’s muscular strength and size is extremely important and a key focus for physiotherapists as it is lost quickly due to inactivity but takes a very long time to come back.
The current ACSM guidelines for increasing strength recommend lifting loads of over 60% of your one rep max (1RM). For physically challenged populations, including the elderly, arthritis sufferers and those post surgery, this load is not possible, one reason is down to pain. Physiotherapist or Sport Specialist are thus left with a bit of a dilemma. Inadequate response by loading to low, or giving a try on the current researched protocol.
4.2) Contraindications
Quite rightly safety of BFR training has also been prevalent in the research community. A survey of over 1800 people performing BFR training reported the most common side effects to be subcutaneous haemorrhage and numbness, which were experienced by 13.1 and 1.3% of participants, respectively. However, these symptoms are often dissipate as the individual becomes more accustomed to this training modality. Reviews by Loenneke have shown BFR training to be a safe and produce similar responses on blood pressure, blood coagulation, delayed onset of muscle soreness (DOMS) and oxidative stress that has been observed during regular resistance training.
Contraindications therefore include a history of deep-vein thrombosis, pregnancy, varicose veins, impaired endothelial function (diabetics included), high blood pressure and cardiac disease.
References
- Kacin A, & Strazar K (2011). Frequent low-load ischemic resistance exercise to failure enhances muscle oxygen delivery and endurance capacity. Scand J Med Sci Sports, 21 , e231-241.
- Wilson JM, Lowery RP, Joy JM, Loenneke JP, & Naimo MA (2013). Practical Blood Flow Restriction Training Increases Acute Determinants of Hypertrophy Without Increasing Indices of Muscle Damage. J Strength Cond Res, epub ahead of print.
- Loenneke JP, Abe T, Wilson JM, Ugrinowitsch C, & Bemben MG (2012) Blood flow restriction: how does it work? Front Physiol, 3, 392.
- Loenneke JP, Wilson JM, Marin PJ, Zourdos MC, & Bemben MG (2012). Low intensity blood flow restriction training: a meta-analysis. Eur J Appl Physiol, 112(5), 1849-1859.
- Loenneke JP, Fahs CA, Wilson JM, & Bemben MG (2011). Blood flow restriction: the metabolite/volume threshold theory. Med Hypotheses, 77(5), 748-752.
- Loenneke JP, Fahs CA, Rossow LM, Abe T, & Bemben MG (2011). The anabolic benefits of venous blood flow restriction training may be induced by muscle cell swelling. Med Hypotheses, 78(1) , 151-154.
- Loenneke JP, Wilson GJ, & Wilson JM (2010) A mechanistic approach to blood flow occlusion. Int J Sports Med, 31(1) , 1-4.
- Schoenfeld, BJ (2013). Potential mechanisms for a role of metabolic stress in hypertrophic adaptations to resistance training. Sports Med, 43(3), 179-194.
- Loenneke JP, Abe T, Wilson JM, Thiebaud RS, Fahs CA, Rossow LM, & Bemben MG (2012) Blood flow restriction: an evidence-based progressive model. Acta Physiol Hung, 99(3) , 235-250.
- Thiebaud RS, Yasuda T, Loenneke JP, Abe T (2013). Effects of low-intensity concentric and eccentric exercise combined with blood flow restriction on indices of exercise-induced muscle damage. Interven Med Appl Sci, 5, 53-59.
- Lowery RP, Joy JM, Loenneke JP, Oliveira de Souza E, Weiner S, McCleary S, & Wilson JM (2013). Practical blood flow restriction training increases muscle hypertrophy during a periodized resistance training program. National Strength and Conditioning Conference, J Strength Cond Res
- Moritani, T., Michael-Sherman, W., Shibata, M., Matsumoto, T., & Shinohara, M. (1992). Oxygen availability and motor unit activity in humans. Eur J Appl Physiol , 64, 552-556.
- Takarada, Y., Tsuruta, T., & Ishii, N. (2004). Cooperative effects of exercise and occlusive stimuli on muscular function in low-intensity resistance exercise with moderate vascular occlusion. Jap J of Physiol , 54, 585-592.
- Takarada, Y., Nakamura, Y., Aruga, S., Onda, T., Miyazaki, S., & Ishii, N. (2000). Rapid increase in plasma growth hormone after low-intensity resistance exercise with vascular occlusion. J Appl Physiol , 88, 61-65.
- Gosselink, K. L., Grindeland, R. E., Roy, R. R., Zhong, H., Bigbee, A. J., Grossman, E. J., et al. (1998). Skeletal muscle afferent regulation of bioassayable growth hormone in the rat pituitary. Appl. Physiol , 84 (4), 1425-1430.
- Fujita, S., Abe, T., Drummond, M., Cadenas, J., Dreyer, H., Sato, Y., et al. (2007). Blood flow restriction during low-intensity resistance exercise increases S6K1 phosphorylation and muscle protein synthesis. Appl. Physiol. , 103, 903-910.
- Yamanaka T, Farley RS, Caputo JL. Occlusion training increases muscular strength in division IA football players. The Journal of Strength and Conditioning Research, 26: 2523-2529.
- Luebbers PE, Fry AC, Kriley LM, Butler MS. The Effects of a Seven-week Practical Blood Flow Restriction Program on Well-trained Collegiate Athletes. J Strength Cond Res, 28(8): 2270–2280.
- Lowery RP, Joy JM, Loenneke JP et al. Practical blood flow restriction training increases muscle hypertrophy during a periodized resistance training programme. Clin Physiol Funct Imaging, 34(4): 317-21.
- Scott BR, Loenneke JP, Slattery KM, Dascombe BJ. Exercise with Blood Flow Restriction: An Updated Evidence-Based Approach for Enhanced Muscular Development. Sports Med, 2014 (epub ahead of print).
- Madarame, H., Neya, M., Ochi, E., Nakazato, K., Sato, Y., & Ishii, N. (2008). Cross-transfer effects of resistance training with blood flow restriction. Sci. Sports Exerc. , 40(2), 258-263.
- Kim, S., Sherk, V., Bemben, M., & Bemben, D. (2012). Effects of Short Term Low Intensity Resistance Training with Blood Flow Restriction on Bone Markers and Muscle Cross-Sectional Area in Young Men. International Journal of Exercise Science. Retrieved from http://digitalcommons.wku.edu/ijes/vol5/iss2/6
- Moore, D. R., Burgomaster, K. A., Schofield, L. M., Gibala, M. J., Sale, D. G., & Phillips, S. M. (2004). Neuromuscular adaptations in human muscle following low intensity resistance training with vascular occlusion. European Journal of Applied Physiology, 92(4-5), 399–406. http://doi.org/10.1007/s00421-004-1072-y
- Loenneke JP, Wilson JM, Wilson GJ, Pujol TJ, Bemben MG. Potential safety issues with blood flow restriction training. Scand J Med Sci Sports, 21: 510-518.
- Loenneke JP, Thiebaud RS, Abe T. Does blood flow restriction result in skeletal muscle damage? A critical review of available evidence. Scand J Med Sci Sports, 25(4): 521-534.
- Nakajima T, Kurano M, Iida H. Use and safety of KAATSU training: results of a national survey. Int J KAATSU Train Res. 2006. 2 (1): 5–13.
- American College of Sports Medicine. Guidelines for Exercise Testing and Prescription (8th ed). Philadelphia, PA: Lippincott Williams & Wilkins, 2009. 65–66.